

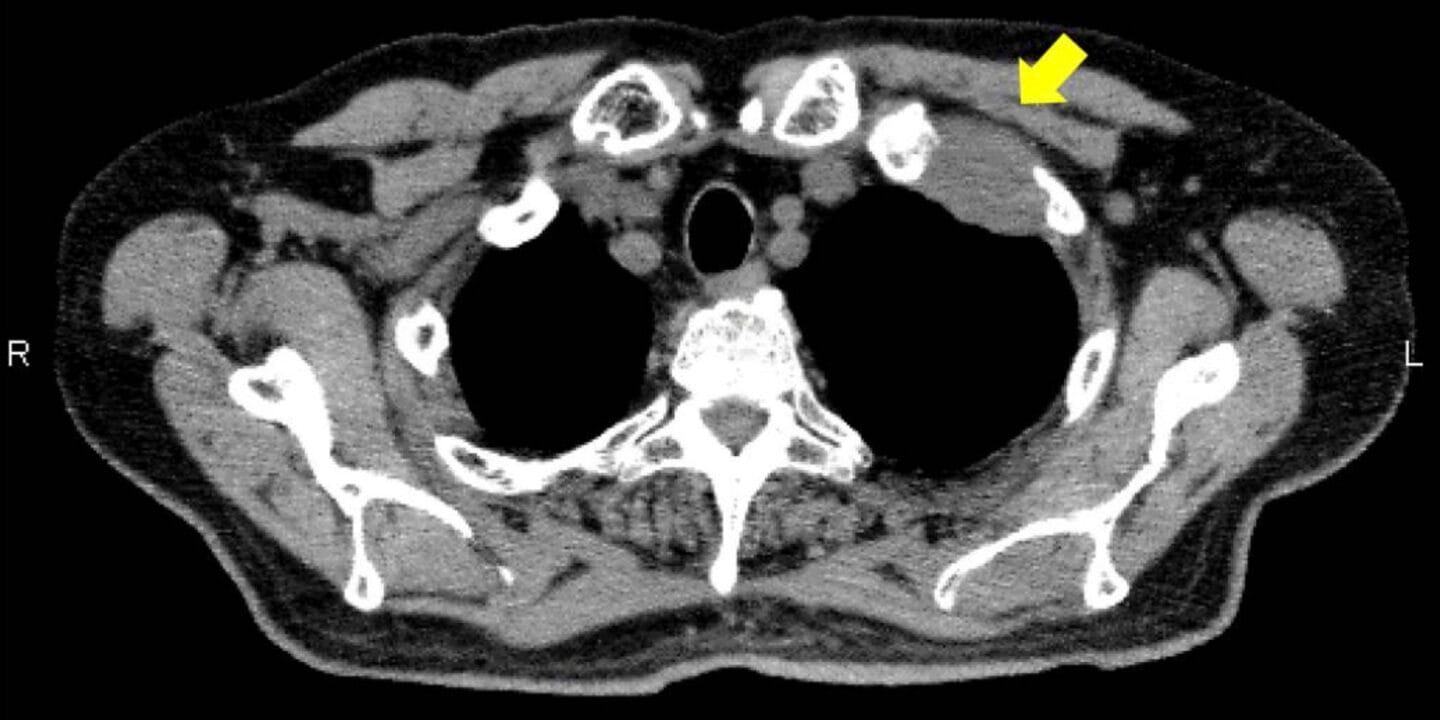
Pancoast tumors are also known as superior sulcus tumors. They are located at the apical pleuro-pulmonary groove, adjacent to the subclavian vessels. They are predominantly non-small cell lung cancers
Clinical features
- *Pancoast syndrome- a cluster of symptoms due to mass effect of the tumor on surrounding structures
- Shoulder pain- the most predominant symptom
- Arm pain
- Horner’s syndrome- ipsilateral ptosis, miosis, enophthalmos, and anhidrosis. Caused by the involvement of the paravertebral sympathetic chain and inferior cervical ganglion
- Weakness and atrophy of muscles of the hand
- Cough, hemoptysis, and dyspnoea occur late in the disease
- Supraclavicular lymphadenopathy and prominent weight loss in a about 30% of cases
Diagnosis
-Core biopsy- preferred
-Bronchoscopy has a low yield because of the peripheral location of these tumors
-Thoracotomy or video-assisted thoracoscopy( VATS) can be used if less invasive methods are nondiagnostic
-Pathology-
- The majority are non-small cell lung cancers
- 5% are small cell
Differential diagnosis
- Lymphoma
- Mesothelioma
- Adenoid cystic carcinoma
- Metastatic cancers
- Vascular aneurysms
- Infections
Staging– TNM
Treatment
Patients with no distant metastasis;
- Concurrent chemoradiotherapy, then
- Tumor resection in those without ME metastases
- Two additional postoperative courses of chemotherapy
- For those who undergo surgical resection, atezolizumab and osimertinib are offered.
Definitive chemoradiotherapy and adjuvant immunotherapy for inoperable, locally advanced disease
Distant metastasis- radiotherapy
Prognostic factors
- Tumor stage
- Horner’s syndrome
- Extension of tumor into the neck base, vertebra, or great vessels
- Involvement of mediastinal lymph nodes
- Longer duration of symptoms










