

A flail chest occurs when three or more adjacent ribs are fractured in 2 or more places, which creates a floating segment that contains the ribs and the soft tissues between them
- The floating segment exhibits paradoxical movement, i.e., it moves in the opposite direction of the normal uninjured chest wall. The detached segment is pulled into the chest wall during inspiration and pushed outward during expiration
- There is increased work of breathing and ultimately compromise in respiratory function
- It is associated with pulmonary contusion, which can cause significant morbidity
- It mainly results from blunt chest trauma; it occurs in 5 to 13% of chest wall injury
- may be difficult to detect clinically in some patients
- Patients have paradoxical movement of the chest wall with breathing, chest wall tenderness, and severe pain on breathing.
- They may exhibit signs of labored breathing
Investigations
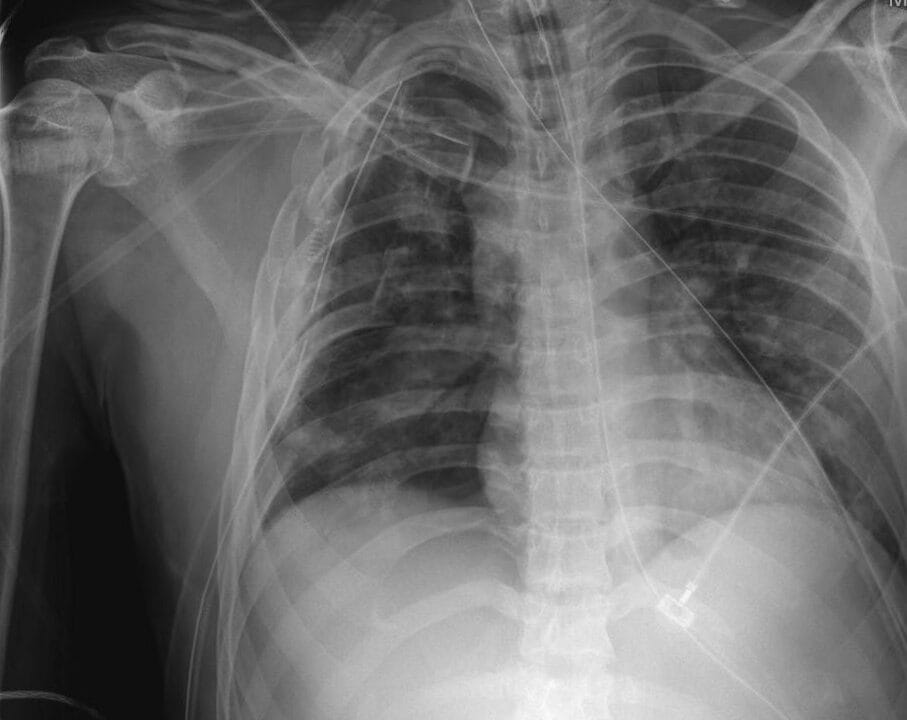
- Chest X-ray- shows the sites of fracture. It may, however, not detect non-displaced fractures.
- May identify pulmonary contusion and other pathologies such as pneumothorax and hemothorax.
- Standard 2D CT scan- highly accurate for the location and number of rib fractures
Management
It is a life-threatening condition and requires immediate care.
- Stabilise the patient first – ABCDEs
- Confirm or rule out other life-threatening conditions
- Pain control
- Oxygen therapy
- Close monitoring for signs of respiratory compromise can be done via a pulse oximeter, capnography, and clinical observation.
- Manual or object pressure is no longer in use as it restricts chest wall expansion.
- Noninvasive positive airway pressure by a mask
- Endotracheal intubation and mechanical ventilatory support for patients with severe injuries, respiratory distress, and worsening respiratory function.
Surgical management-
- In Patients with flail chest, early operative management reduces pulmonary complications, facilitates ventilator weaning, and shortens mechanical ventilation time.
- However, it is of little benefit in those with associated pulmonary contusion.
- The procedure is performed within 48 hours of injury.
- Fixing all ribs is not necessary, but in general, ribs 4 to 9 should be repaired because they provide the majority of the stability to the chest wall.
- The standard approach is fixation using titanium plates placed outside the chest wall and secured using locking screws.
- A chest tube may be required if the pleura is violated during fixation.
- Adjunctive techniques: iliac bone graft, demineralized bone matrix










