- Home
- INTERNAL MEDICINE
- Iron Deficiency Anaemia


Iron deficiency Anaemia occurs when iron losses or physiological requirements exceed absorption.
Aetiology
- Increased physiologic demand, e.g. in infancy, puberty and pregnancy.
- Decreased supply – dietary deficiencies.
- Cow’s milk (infants), ‘tea and toast’ diet(elderly)
- Post-gastrectomy
- Malabsorption (IBD of the duodenum, celiac disease, autoimmune atrophic gastritis)
- Increased losses
- Haemorrhage
- Obvious causes: Menorrhagia, AUB, Frank GI bleeding
- Occult: PUD, Gastric or colorectal malignancy, hookworm infestation.
- Hemolysis
Clinical Presentation
- Fatigue may present before clinical anaemia.
- S/s of anaemia: Decreased exercise tolerance, headache, dizziness, palpitations, oedema.
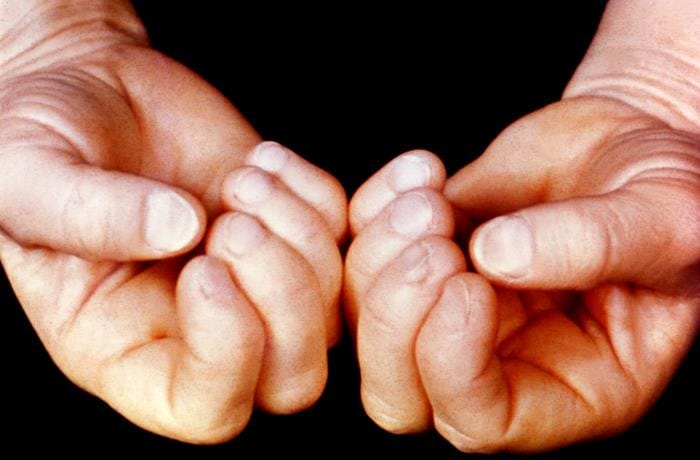
- Brittle hair, nail changes (koilonychia, brittle nails)
- Pica
- Restless leg syndrome
Investigations
Confirmation of iron deficiency
- Iron indices. Low serum ferritin, low serum iron, high TIBC, low Transferrin saturation, and high soluble transferrin receptor.
- FHG, PBF – low Hb, microcytic hypochromic picture, anisocytosis, target cells.
- BMA
Investigating for the cause: OGD and Colonoscopy; stool for O/C
Treatment
- Treat underlying cause
- Transfusion if Hb <6g/dl and patient symptomatic.
- Iron supplementation
- Oral.
Ferrous sulphate 200mg TDS (195mg elemental iron/day), Ferrous gluconate 300mg BD (70mg elemental iron/day)
Duration: 3-6 months and taken with vitamin C to enhance absorption.
- IV is used if the patient cannot tolerate or absorb oral iron, continuing blood loss, or CRF on dialysis.
Iron sucrose, iron dextran, iron isomaltose, iron carboxymaltose.
- Monitor response.










