

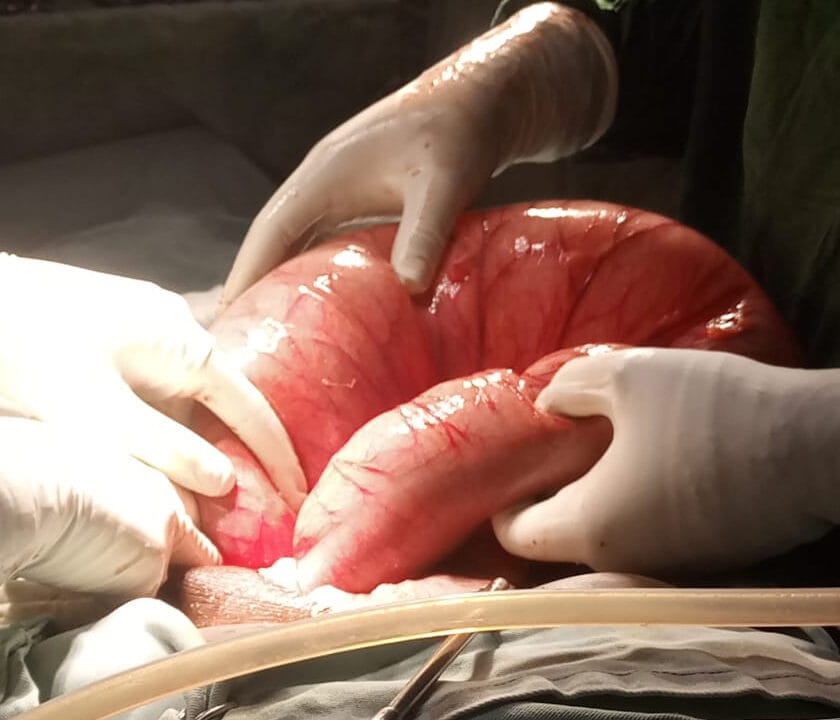
Sigmoid volvulus is a common cause of intestinal obstruction. Volvulus refers to the torsion of a segment of the alimentary canal.
Pathophysiology;
When an air-filled loop of bowel twists anticlockwise about its mesentery. Obstruction of the lumen occurs at 180⁰ while vascular compromise occurs at 360⁰
Risk factors
1. Anatomic factors
- Long redundant sigmoid colon with narrow mesenteric attachment
- Chronic constipation
- Longer sigmoid colon in males
- Decreased pelvic space- pregnancy, pelvic mass
2. Colonic dysmotility
- Prolonged colonic transit
- Children with Hirschsprung disease
Clinical presentation
- There is slow progressive abdominal pain, distention, nausea, and constipation. The pain is continuous and severe and becomes colicky during peristalsis. Vomiting occurs days after the onset of pain.
- Patients present 3 or 4 days after symptom onset
Physical examination
- Abdominal distension
- Tympanicity, tender to palpation
- Emptiness in the left iliac fossa in some
- Fever, hypotension, tachycardia, guarding, rigidity, and rebound tenderness are signs of peritonitis or a perforation
- Younger patients may have a history of recurrent attacks which resolve due to detorsion
Diagnosis – established by imaging
Investigations
1. CBC, electrolytes, lactate, and urinalysis
2. PDT to rule out pregnancy
3. In those with suspected perforation – serum amylase, lipase, aminotransferases, ALP, and bilirubin to rule out other causes of acute abdomen
- In uncomplicated sigmoid volvulus, all lab findings are normal.
4. CT scan – bird beak appearance and whirl pattern. The absence of rectal gas and split wall sign are other features.
- Loss of bowel enhancement, pneumatosis intestinalis, portal venous gas – bowel necrosis
5. Abdominal Xray- coffee bean appearance, bent inner tube appearance
- The presence of free intraperitoneal gas shows perforation
- It is not diagnostic in 40 % of cases
6. Contrast enema – bird beak configuration or twisted taper appearance
Differential diagnosis
- Intestinal pseudo-obstruction
- Toxic megacolon
Management
1. Patient with alarm signs- immediate surgical management
2. Patient without alarm signs
a) Flexible sigmoidoscopy- in an attempt to detorse the twisted segment. If successful, surgery should be done on the same admission or shortly after due to the high risk of recurrence and increased mortality with recurrent sigmoid volvulus
- If endoscopic detorsion fails, refer for urgent surgical management
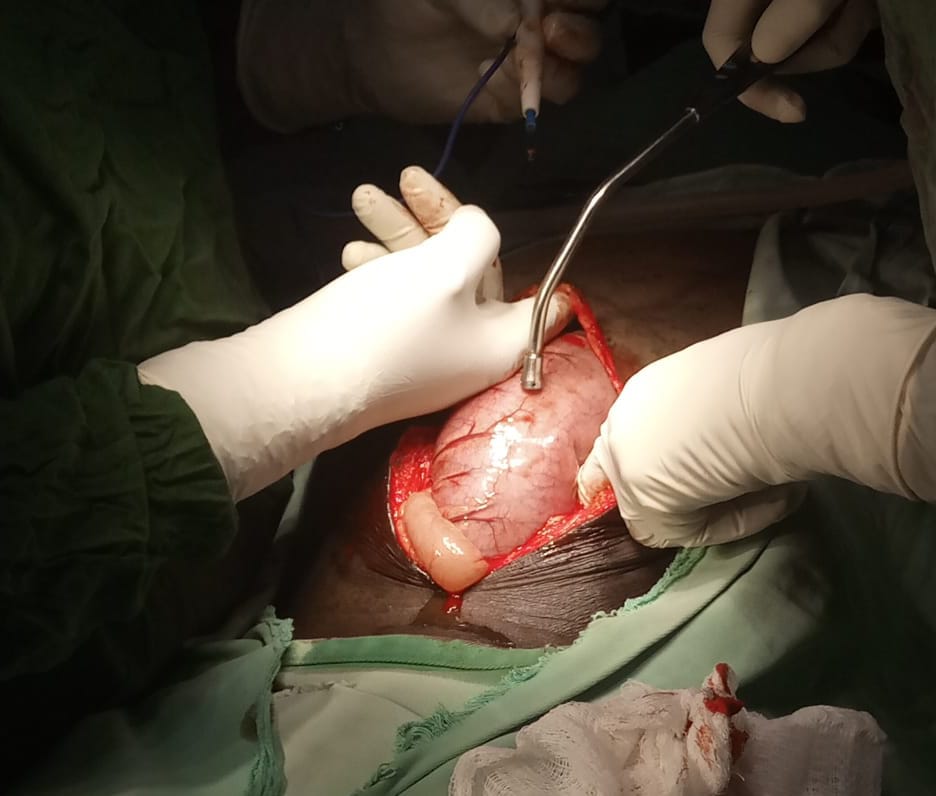
b)Surgery;
- Resection and primary colorectal anastomosis. A colostomy may be considered on a case-by-case basis.
- Nonresectional surgery is not recommended due to the high risk of recurrence.
-There is a limited role for nonoperative management
Prognosis– mortality is most increased in those who have developed gangrene
Complications
- Bowel necrosis
- Fecal peritonitis and septic shock
- Recurrence
- Bowel obstruction










