

Esophagitis is an inflammation of the oesophagal mucosa.
Aetiology;
1. Gastroesophageal reflux disease( GERD) is the leading cause. The oesophagal mucosa is exposed to gastroduodenal contents for prolonged periods
Factors involved in the development of GERD include;
- Abnormalities of the lower oesophagal sphincter
- Hiatus hernia
- Delayed oesophagal clearance
- Increases gastric acid exposure time
- Defective gastric emptying
- Raised intra-abdominal pressure
- Patient factors- visceral sensitivity and patient vigilance
- Diet- fat, alcohol, tea, and coffee relax the lower oesophagal sphincter and may cause symptoms
2. Infections- candidiasis, herpes, CMV infection
3. Corrosives- ingestion of strong bleach and battery acid
4. Drugs- potassium supplements, NSAIDs, bisphosphonates and antibiotics such as tetracyclines
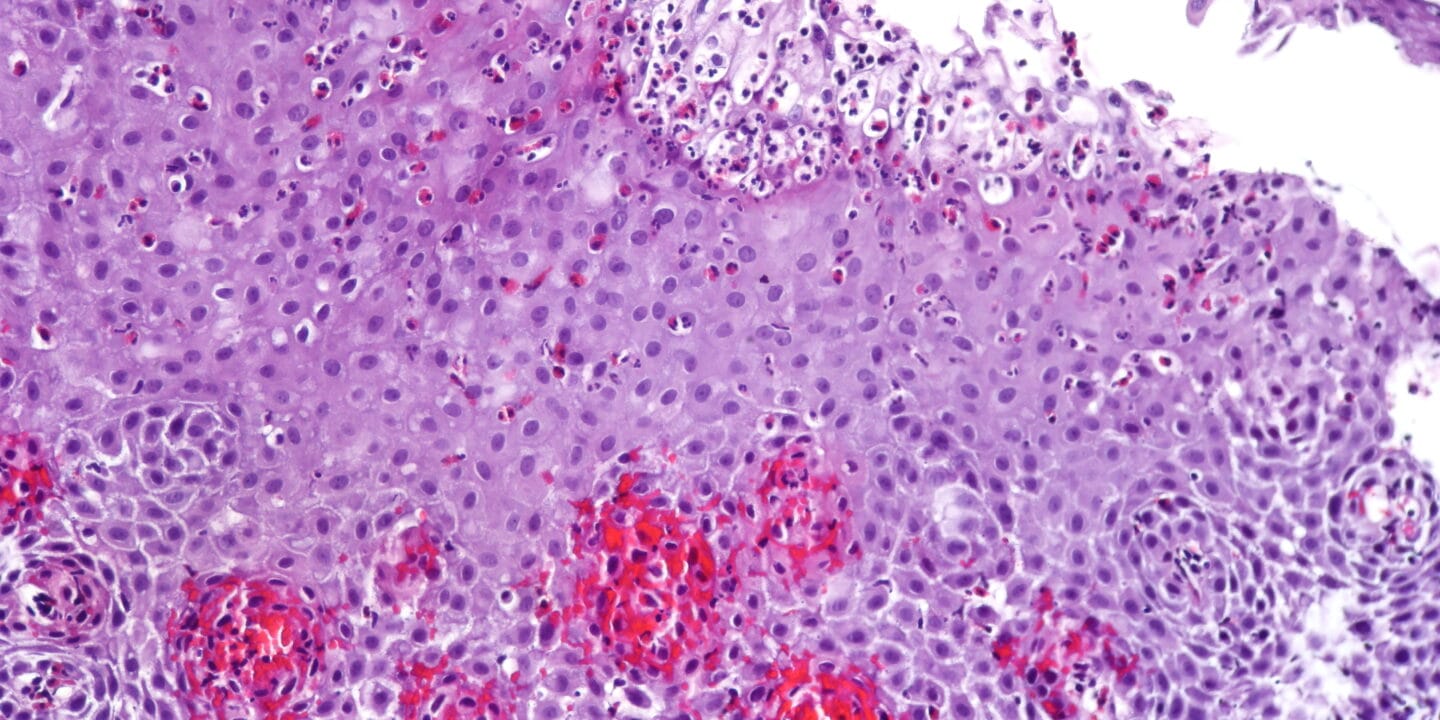
5. Eosinophilic esophagitis-
- more common in children
- It occurs more often in atopic individuals.
- Characterized by eosinophilic infiltration of the oesophagus
6. Immune-mediated disorders- Crohn’s disease, graft vs host disease
7. Others- achalasia, muscular dystrophy, radiotherapy
Clinical presentation
1. GERD- heartburn, and regurgitation are major
- Waterbrash- salivation due to reflex salivary gland stimulation
- The patient is often overweight
- Choking at night awakens the patient
- Odynophagia or dysphagia may be present
- Atypical chest pain
- Hoarseness of voice
- Recurrent chest infections, chronic cough, asthma
2. Esophageal candidiasis is more common in debilitated patients, HIV patients and those taking broad-spectrum antibiotics or cytotoxics
3. Corrosives- may present with painful burns to the mouth and pharynx
- Oesophageal perforation and mediastinitis may occur
4. Drugs- NSAIDs and potassium supplements may cause ulcers when tablets are trapped above a stricture
5. Eosinophilic esophagitis- dysphagia or foods bolus obstruction,
- Heartburn, chest pain and vomiting may be present
Investigations
-Recommended if patients present over the age of 55, symptoms are atypical or if a complication is suspected in the setting of GERD
-Endoscopy- investigation of choice
- A negative result in someone with compatible symptoms, still treat for GERD
-24-hour pH monitoring- when considering surgical intervention or the diagnosis is unclear. a pH of less than 4 for more than 6 to 7% of the study time is diagnostic of GERD
- Impedance testing is an alternative
-In eosinophilic esophagitis, endoscopy is usually normal, but mucosal rings, strictures or a narrowed oesophagus may be seen
Management
1. GERD-
-Lifestyle advice- weight loss, the elevation of bed head in those who have nocturnal symptoms, avoidance of foods that worsen symptoms, avoidance of late meals, smoking cessation
-PPIs – for those who fail lifestyle modification measures. Relieve symptoms and cure esophagitis
- Effective
- Recurrence is common when medication is stopped; some require lifelong treatment
-Domperidone- in those with dysmotility
-Antacids and alginates improve symptoms
-H2 receptor antagonist- for relief but not cure
*H pylori eradication has no value. However, it is advised for those who require PPIs for more than one year
-Laparoscopic antireflux surgery-
- Those who don’t respond to medical therapy, those unwilling to take long-term PPIs and those with severe regurgitation
- Complications of surgery- abdominal bloating, inability to vomit
Other causes;
-Treat infections
-Corrosives- analgesia, nutritional support
- Barium swallow demonstrates the extent of stricture; done after the acute phase.
- Endoscopic dilatation
-Drugs- use liquid preparations of NSAIDs and potassium supplements in patients with strictures. Cautious use of bisphosphonates in those with oesophagal disorders
-Eosinophilic esophagitis-
- Initially- Children- elimination diets; Adults- PPIs
- Topical glucocorticoids, e.g. fluticasone, for 8 to 12 weeks. Administered via a metered-dose inhaler. The patient sprays into the mouth and swallows
- Montelukast, if refractory symptoms occur
Complications
- Oesophageal perforation
- Mediastinitis
- Barrett’s oesophagus
- Adenocarcinoma
- Anaemia
- Oesophagal stricture
- Gastric volvulus










