

Otitis Media (OM) refers to inflammation of the middle ear, commonly seen in both children and adults. It can occur as a result of infections or other causes, leading to a range of symptoms and potential complications.
Etiology
Otitis media can be classified into different types based on its cause, duration, and presence of infection. The main etiological factors include:
- Infectious Agents:
- Bacterial Infections: Common organisms include:
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
- Viral Infections: Common viruses include respiratory syncytial virus (RSV), influenza virus, and rhinovirus. Viral infections may precede bacterial infections.
- Bacterial Infections: Common organisms include:
- Non-infectious Causes:
- Eustachian Tube Dysfunction: Poor function of the eustachian tube can lead to negative middle ear pressure and fluid accumulation, creating an environment conducive to infection.
- Allergies: Allergic rhinitis can contribute to eustachian tube dysfunction and subsequent middle ear inflammation.
- Environmental Factors: Exposure to secondhand smoke, air pollution, and changes in atmospheric pressure can increase the risk.
Classification
Otitis media can be classified into several types:
- Acute Otitis Media (AOM):
- Definition: A rapid-onset infection of the middle ear, often accompanied by acute symptoms.
- Duration: Symptoms last less than 3 weeks.
- Otitis Media with Effusion (OME):
- Definition: Presence of fluid in the middle ear without signs of acute infection. Commonly follows AOM.
- Duration: Can persist for weeks to months, potentially leading to hearing loss.
- Chronic Otitis Media:
- Definition: A chronic infection characterized by persistent inflammation, perforation of the tympanic membrane, and possible fluid drainage.
- Duration: Symptoms last more than 3 months.
- Recurrent Otitis Media:
- Defined as three or more episodes of AOM within six months or four episodes in a year.
Epidemiology
- Otitis media is one of the most common childhood infections, particularly between the ages of 6 months and 2 years.
- The incidence decreases after age 2, but it can still occur in older children and adults.
- Risk factors include younger age, family history, daycare attendance, and the presence of siblings.
Clinical Features
- Signs and Symptoms:
- Acute Otitis Media:
- Ear pain (otalgia) is often the most prominent symptom.
- Irritability, difficulty sleeping, and poor feeding in infants.
- Fever may be present.
- Hearing loss and drainage from the ear if there is a perforation.
- Otitis Media with Effusion:
- Often asymptomatic but may present with mild discomfort, hearing loss, or a sensation of fullness in the ear.
- Acute Otitis Media:
- Physical Examination:
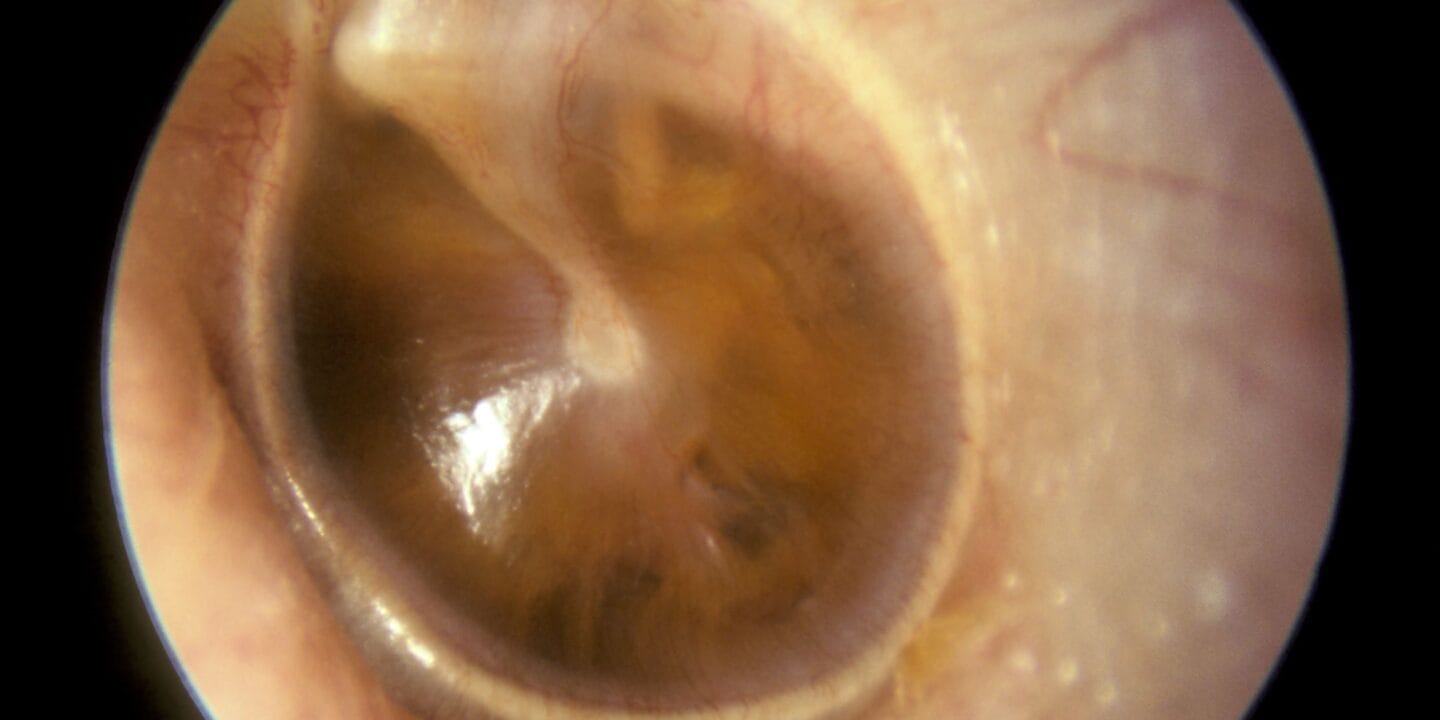
- Otoscopy: Redness, bulging, and loss of landmarks on the tympanic membrane are indicative of AOM. In OME, the tympanic membrane may appear retracted or have fluid levels.
Diagnosis
- Clinical Diagnosis:
- Diagnosis is primarily clinical, based on history, symptoms, and otoscopic examination.
- The presence of fluid in the middle ear, combined with signs of infection, supports the diagnosis of AOM.
- Imaging Studies:
- Mastoid CT Scan: May be indicated in complicated cases or when there are concerns for mastoiditis or other intracranial complications.
- Tympanometry: Useful in assessing middle ear function and fluid presence, especially in cases of OME.
Management
- Acute Otitis Media:
- Observation: In cases of mild symptoms and in children older than 2 years, a period of observation for 48-72 hours may be appropriate before initiating antibiotics.
- Antibiotic Therapy: First-line treatment typically includes:
- Amoxicillin: 80-90 mg/kg/day in divided doses for 5-7 days.
- Consideration for high-dose amoxicillin-clavulanate (Augmentin) in recurrent or severe cases.
- Symptomatic Relief: Analgesics (e.g., acetaminophen or ibuprofen) to relieve pain and fever.
- Otitis Media with Effusion:
- Watchful Waiting: Most cases resolve spontaneously; management focuses on monitoring.
- Surgical Intervention: Consider tympanostomy tube placement if OME persists for more than 3 months, leads to significant hearing loss, or causes recurrent infections.
- Chronic Otitis Media:
- Medical Management: Includes cleaning the ear and antibiotics for active infection.
- Surgical Intervention: Surgical repair of tympanic membrane perforation or mastoidectomy may be required.
Prognosis
- The prognosis for AOM is generally good, with most children recovering completely with appropriate treatment.
- OME may resolve spontaneously but can lead to temporary hearing loss or developmental delays if not managed appropriately.
Complications
- Acute Complications:
- Mastoiditis: Infection of the mastoid air cells, requiring aggressive treatment and possible surgical intervention.
- Perforation of the Tympanic Membrane: May occur, leading to persistent otorrhea.
- Chronic Complications:
- Chronic Otitis Media: Prolonged infection may lead to persistent drainage and hearing loss.
- Hearing Loss: Resulting from OME or chronic infections can impact language and developmental milestones in children.
- Intracranial Complications: Rare but serious complications include meningitis, brain abscess, and venous sinus thrombosis.










