- Home
- INTERNAL MEDICINE
- Megaloblastic Anemia


Megaloblastic anemia is caused by folic acid or vitamin B12 deficiency and problems with folic acid metabolism.
Erythroblasts with late nuclear maturation due to flawed DNA synthesis are found in the bone marrow in megaloblastic anemia. Megaloblastic changes also occur in myelodysplasia due to dyserythropoietic treatment involving DNA synthesis-interfering medications (e.g., azathioprine and hydroxyurea).
Clinical features of megaloblastic anemia
Symptoms
- Visual disturbance
- Shortness of breath
- Impotence
- Impairment of memory
- A feeling of discomfort or unease
- Abnormal sensation
- A change in personality
- Hallucinations
- Depression
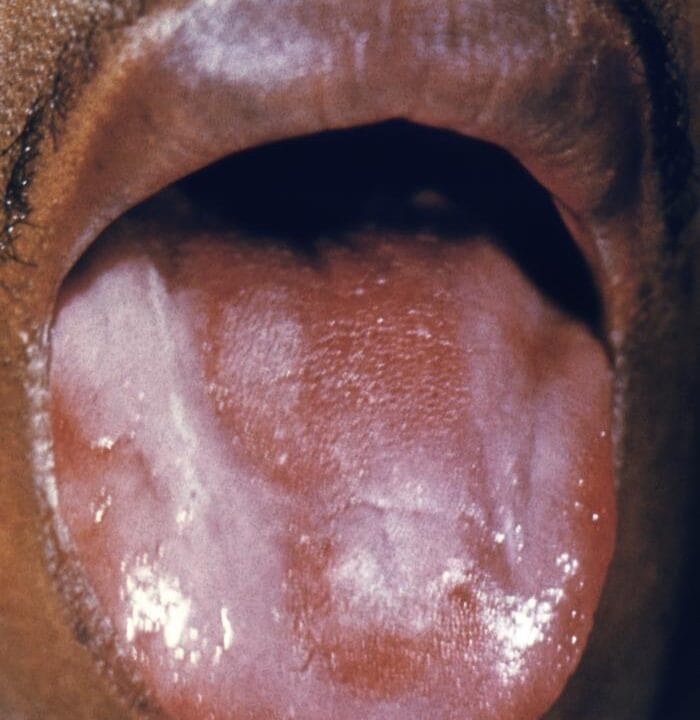
Signs
- Angular cheilosis
- Cardiac failure
- Vitiligo
- Smooth tongue
Investigations
- Hemoglobin (reduced )
- Elevated MCV (> 120 fL)
- Low red cell count
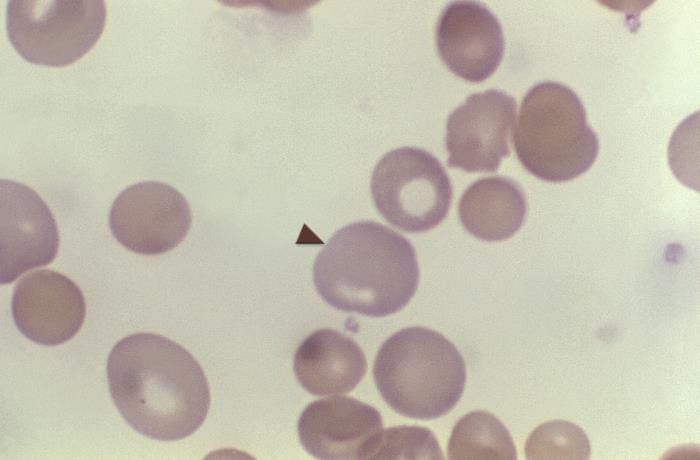
- neutrophil hypersegmentation and erythrocyte fragmentation may be seen on a blood film
- Increased cellularity and megaloblastic changes in erythroid series in bone marrow examination
- Increased ferritin levels
Vitamin B 12 deficiency
Vitamin B12 is a cofactor for two essential human reactions critical during DNA synthesis. All meals with an animal origin contain it. If all consumption or absorption suddenly stops, it typically takes more than three years for a deficit to develop since the body maintains sufficient stores of vitamin B12.
Causes
- Reduced ileal absorption because of surgical resection
- Reduced synthesis of intrinsic factors following gastrectomy
- Destruction of intrinsic factor in pernicious anemia
- Helicobacter pylori infection
- Competition in the intestine by bacteria in blind loop syndrome
- Pancreatic insufficiency
- Dietary deficit
Diagnosis
- Macrocytic anemia
- Megaloblastic smear
- Low serum levels of vitamin B12
Treatment
- Hydroxocobalamin 1mg administered intramuscularly to a maximum of 5-6 mg over three weeks,
- after which there will be lifetime maintenance therapy at 1000 mg every three months.
Folate deficiency
The leading cause is poor intake. There is roughly 5 mg of folic acid stored in the body, sufficient to meet needs for two to three months. Green vegetables like spinach, broccoli, and offal contain folate.
Causes
- Rising demand, for example, in pregnancy
- Nutritional deficiency
- Tropical sprue
- Excessive losses, for example, during hemodialysis.
- Medications such as phenytoin that decrease absorption
Diagnosis
- Macrocytic anemia
- Megaloblastic blood smear
- Reduced serum levels of folic acid
- Normal serum levels of vitamin B12.
Treatment
- Folic acid 5 mg PO for 21 days
- followed by maintenance therapy at 5 mg once per week.
- All women intending to become pregnant should take 400 mg of prophylactic folic acid daily.