- Home
- INTERNAL MEDICINE
- Myocarditis


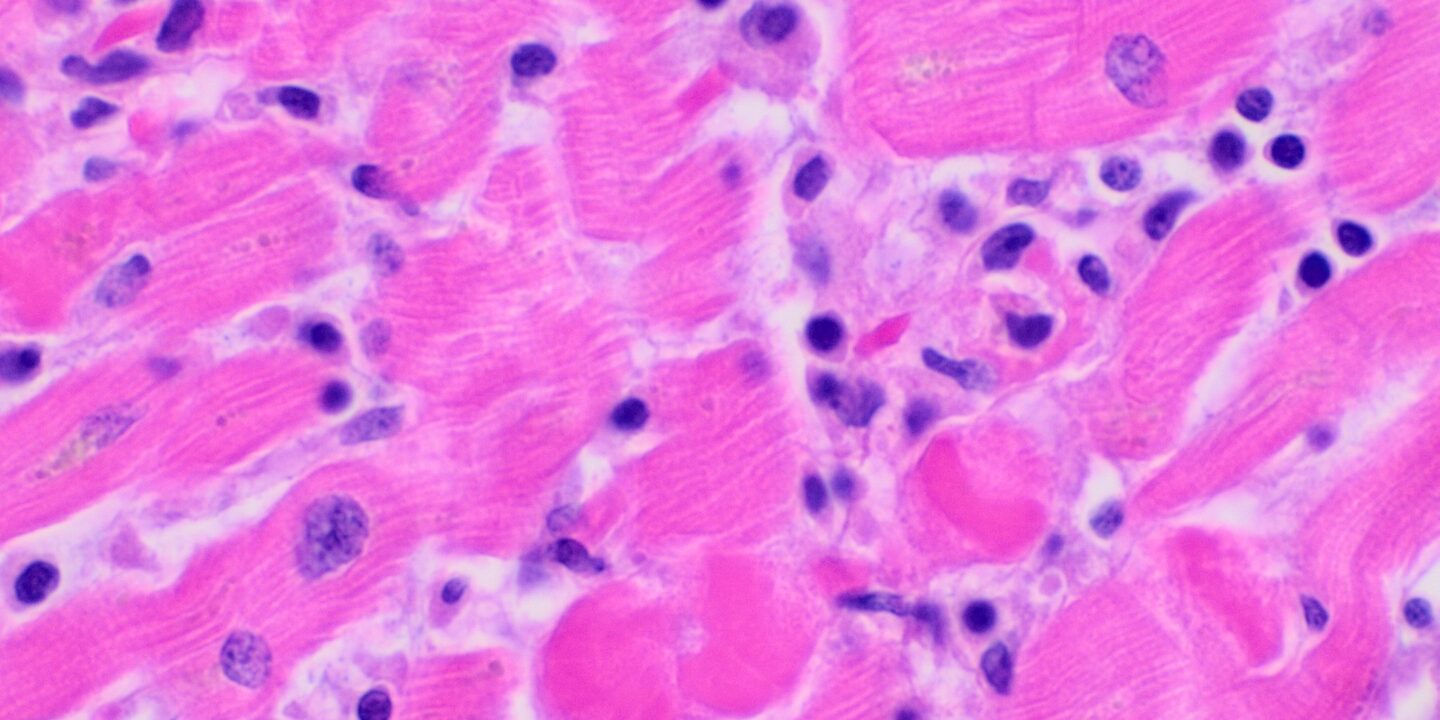
Myocarditis is an acute inflammation of the cardiac muscle. It may present with focal or diffuse involvement of the myocardium. Viral infections are the most common cause, such as influenza A virus and Coxsackie virus.
Susceptibility after a viral infection is increased by;
- Immunosuppression
- Glucocorticoid use
- Radiation
- Previous myocardial damage
- Exercise
Etiology
1. Infections;
- Viral- Influenza A and B, Coxsackie, HIV, adenovirus
- Bacterial- Lyme disease, Mycoplasma pneumoniae
- Protozoal- Toxoplasma gondii, Chaga’s disease
- Fungal- Aspergillus
- Parasitic- Schistosomiasis
2. Autoimmune;
- SLE, rheumatoid arthritis, sarcoidosis, systemic sclerosis
- Hypersensitivity to penicillins, sulphonamides, lead, carbon monoxide
3. Drugs;
- Alcohol, cocaine, lithium, clozapine anthracylines
Clinical presentation
It can present in one of four ways;
1. Acute myocarditis- presents over a relatively long period with heart failure. May lead to dilated cardiomyopathy
2. Fulminant myocarditis- results in severe heart failure or cardiogenic shock. It follows a viral or influenza-like illness
3. Chronic active myocarditis- associated with chronic myocardial inflammation
4. Chronic persistent myocarditis- defined by focal myocardial infiltrates. it can cause chest pain and arrhythmias
- It is a reported cause of sudden cardiac death, especially in athletes
- Causes of death are ventricular arrhythmias and rapidly progressing heart failure
- Cardiomyopathy is a sequel in some cases
Investigations
- Echocardiogram- left ventricular dysfunction may be present
- Diagnostic cardiac MRI- may show myocardial inflammation or infiltration
- ECG- is abnormal, but changes are nonspecific.
- Serum troponins and creatine kinase- may be elevated in the early phase
- Endomyocardial biopsy- for confirmation
- BNP or NT-proBNP- if heart failure is suspected
- Others- CBC, acute phase reactants
Management
Is mainly supportive
- Patient to avoid intense physical exertion as this could cause life-threatening arrhythmias
- Alcohol restriction
- Those with heart failure should receive standard therapy for heart failure
- Hemodynamically stable with reduced ejection fraction- diuretics, ACE inhibitors, beta-blockers add mineralocorticoid receptor antagonist if symptomatic with an ejection fraction of less than 35%
- Therapy for arrhythmias – is generally supportive since they resolve after the acute phase of the disease
- Anticoagulation in the presence of systemic embolism or acute left ventricular thrombus
- Avoid NSAIDs
- Specific antimicrobial therapy if the cause is identified
- Rarely is cardiac transplantation may be required
Prevention
- Vaccination for some forms of viral myocarditis
- Infection control










