- Home
- INTERNAL MEDICINE
- Aortic Dissection


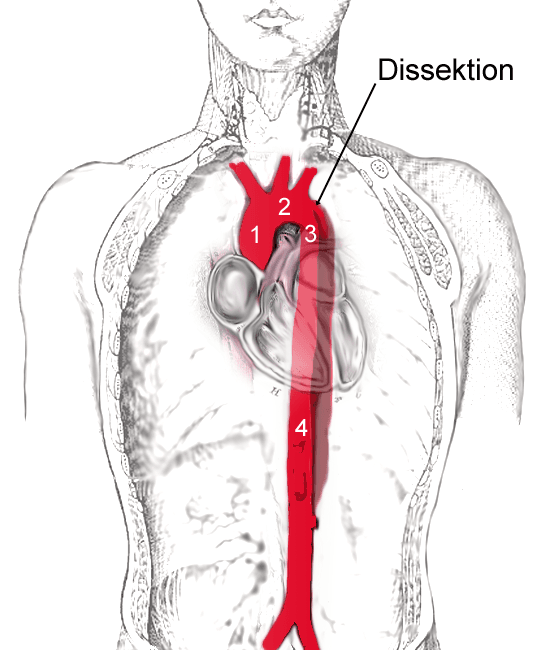
Aortic Dissection is a break in the integrity of the wall (intima)of the aorta allowing blood into the media, which is subsequently torn into 2, creating another lumen alongside an already existing lumen. May lead to damage of the aortic valve and compromise of aortic branches.
Eventually, the new false lumen joins with the true lumen to create a double-barreled aorta. Alternatively, it may burst into the pericardium or the left pleural cavity, a fetal occurrence.
Some dissections are due to primary bleeds in the media, which rupture into the true lumen through the intima. Chronic arterial dissections may eventually cause aortic aneurysms, and at the same time, aneurysms may complicate dissection.
Divided into type A which involves the ascending aorta, and type B, which does not.
Risk Factors
- Atherosclerosis
- Hypertension (most common)
- Genetic- Ehlers-Danlos and Marfan’s syndromes
- Previous cardiac surgery-aortic valve replacement, CABG
- Fibromuscular dysplasia
- 3rd-trimester pregnancy
- Trauma
- Iatrogenic-Intra aortic balloon pumping and cardiac catheterization
Clinical Features
1. – Chest pain(anterior)- ascending aorta involvement
– Back pain(intracapsular)- descending aorta involved
– Pain is tearing, sudden in onset, and associated with collapsing
2. Hypertension- unless in the case of massive
bleeding
3. Asymmetry of carotid, femoral or brachial pulses with signs pointing to regurgitation of the aorta
4. Occlusion of coronary arteries may lead to mi, carotid to stroke, spinal to paraplegia, coeliac and mesenteric to acute abdomen due to mesenteric ischemia, renal to renal failure, and if leg arteries top acute limb ischemia
Investigations
- MRI/CT angiography is the gold standard- demonstration of the double-barreled aorta
- Chest x-ray – aortic knuckle disruption and upper mediastinal broadening, pleural effusion (left side)
- ECG –hypertrophy of the left ventricle, inferior MI-related changes
- Doppler echo-aortic root dilatation, regurgitation of aorta, dissection flap
- TOE – since transthoracic echo only shows the first three to four cm of the aorta(ascending)
Management
- Urgent treatment due to high rates of early mortality
- Start with antihypertensive and analgesics
- Type A: surgery as an emergency to replace ascending aorta
- Type B: medical management unless in the case of impending or actual external rupture, or ischemia of vital organs, since surgery-related mortality is high
- Aims to maintain MAP at 70-75 mmhg to lower the force of blood ejection from the left ventricle
- First-line therapy with β –blockers, labetalol used since it has α blockade too
- Calcium channel blockers like diltiazem and verapamil are used if β –blockers are contraindicated
- If the above fails to control BP, use sodium nitroprusside
Use of percutaneous repair of endolumen- fenestrates intima flap to allow the return of blood to the true lumen, or alternatively implanting a graft stent from the femoral artery.










