- Home
- INTERNAL MEDICINE
- Yellow Fever



Yellow Fever is a viral hemorrhagic fever that is caused by the yellow fever virus, a flavivirus. Mosquito-borne. Endemic in South America and sub-Saharan Africa. The vaccine is protective against all strains. Mortality is 15%.
Causes injury to hepatocytes, myocardium, and kidney and cause circulatory shock. Infectivity- in viremic phase; 3 to 6 days after the bite and lasts 4 to 5 days.
Causes of Yellow Fever
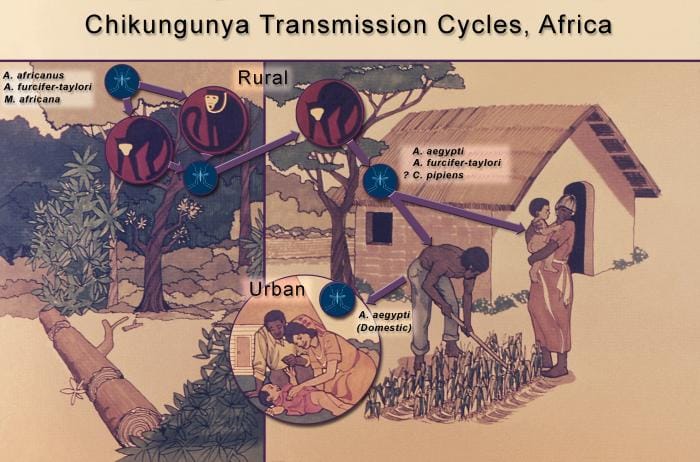
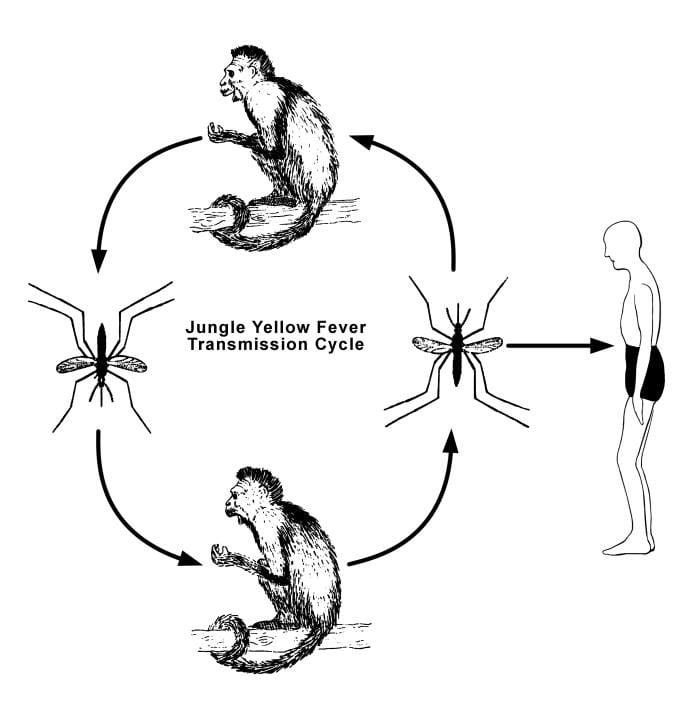
Infection to humans
- When trees are felled or when monkeys raid human settlements.
- Human-to-human transmission is possible.
Clinical presentation of Yellow Fever
Three stages;
1. Infection
- Fever, malaise, headache, anorexia, myalgia, dizziness
- Epigastric tenderness, reddening of conjunctiva and gums
- Tender hepatomegaly
2. Remission
- 48 hours after 1st phase
- Reduction of fever and symptoms
- 15% persist to stage 3
3. Intoxication
- A return of fever, epigastric pain, jaundice, nausea and vomiting, hemorrhagic diathesis
- Multi-organ failure
Differential diagnosis of Yellow Fever
- Malaria
- Typhoid
- Viral hepatitis
- Aflatoxin poisoning
- Leptospirosis
- Hemorrhagic fevers
Diagnosis
- Detection of the virus through culture or PCR-first 3 to 4 days
- Serology- IgM or a four-fold rise in IgG
- Full blood count- leucopenia
- Immunohistochemistry- for viral antigens
- Postmortem findings- acute mid-zone necrosis of liver and councilman bodies
Management of Yellow Fever
Supportive is the mainstay.
- Nutrition
- Prevent hypoglycemia
- Treat hypotension
- Oxygen and anticonvulsants
- Fresh frozen plasma for bleeding and dialysis for renal failure
- Manage metabolic acidosis, prevent gastric distention and aspiration
- Isolation.
- ICU care
Prevention
Vaccination- protective for 10 yrs
- When travelling to an endemic area
- Side effects; hypersensitivity, encephalitis, viscerotropic disease
- Contraindicated in; severely immunocompromised and egg allergy